
 It was shown in this blog that for centuries manipulation techniques were a matter of
It was shown in this blog that for centuries manipulation techniques were a matter of continuity between one generation of manipulators to the next (Wiese and Callender, 2010). However, right at the end of 19th century yet another profession rose to establish itself as a valid approach to rehabilitation. Four nurses in Great Britain founded what would later be known as the Chartered Society of Physiotherapy. Those nurses initially sought to offer treatment to polio patients and British soldiers through massage and joint mobilization. By forming this society they took up the challenge of protecting that fledgling profession and imprint it in the minds of patients and clinicians (Pettman, 2007). Soon United States of America followed in the registration of Physical Therapists as a professional organization, while the pre-World War I saw the establishment of physiotherapy schools in New Zealand, U.S.A. and Australia (Bialosky et al., 2012).
continuity between one generation of manipulators to the next (Wiese and Callender, 2010). However, right at the end of 19th century yet another profession rose to establish itself as a valid approach to rehabilitation. Four nurses in Great Britain founded what would later be known as the Chartered Society of Physiotherapy. Those nurses initially sought to offer treatment to polio patients and British soldiers through massage and joint mobilization. By forming this society they took up the challenge of protecting that fledgling profession and imprint it in the minds of patients and clinicians (Pettman, 2007). Soon United States of America followed in the registration of Physical Therapists as a professional organization, while the pre-World War I saw the establishment of physiotherapy schools in New Zealand, U.S.A. and Australia (Bialosky et al., 2012).
Since the profession’s inception, manipulative therapy has been a component of the physical therapist practice (Bialosky et al., 2012). Manipulation was for centuries the domain of empirics, yet in less than 50 years it became a treatment provision by organized professional groups and societies (Evans, 2010).
As we now know, physiotherapy emerged at about the same period as osteopathy, chiropractic, and the contemporary, reasoned and now more “scientific” medical profession. However, the paths of those professions would eventually differ in many ways. Osteopathy would merge with the medical profession, while chiropractic would adapt an autonomous form that would eventually be highly competitive with medicine. The origin of physiotherapy, on the other hand, always contained a significant degree of collaboration with medical practitioners and so it is hitherto (Pettman, 2007).
During the passing of only half a century after the profession’s establishment, physiotherapists from around the globe were beginning to research the essential beliefs of their practice and try to organize and develop the reasoning behind their clinical applications (Pettman, 2007). At the same time, it is a well-known fact that in the first decades of the 20th century, recognized and fully qualified educators of both American and British Schools of Osteopathy provided mentorship, guidance and valuable training to physiotherapists (Huijbregts, 2010; Pettman, 2007).
This fact led to the development of physiotherapy and allowed at a handful, pioneer individuals to distinguish themselves, influence the entire profession and consequently elevate manipulation to a standard level of practice and reasoning. This attained clinical level would accompany physiotherapists into the future and, in my opinion it will as well, for all coming times.
To begin with, James Mennel and James Cyriax (among others) heavily influenced the clinical reasoning and the decision making in the practice of physiotherapy (Bialosky, 2012). Mennel explained in detail how thoracic spinal symptoms are mimicking true visceral symptoms thus highlighting the need for extra attention in the interpretation of pain relief after spinal manipulation. Additionally Cyriax, in his 1954 book “Textbook of Orthopaedic Medicine, Volume I” explained in detail the “selective tension tissue testing” which is a method of logical clinical reasoning and differential diagnosis (Pettman, 2007). But this was only the beginning. A chain reaction commenced and those orthopaedic physicians, apart from the practice of manipulation itself, influenced the clinical decision making of those who would come to succeed them (Paris, 2006, 2000).
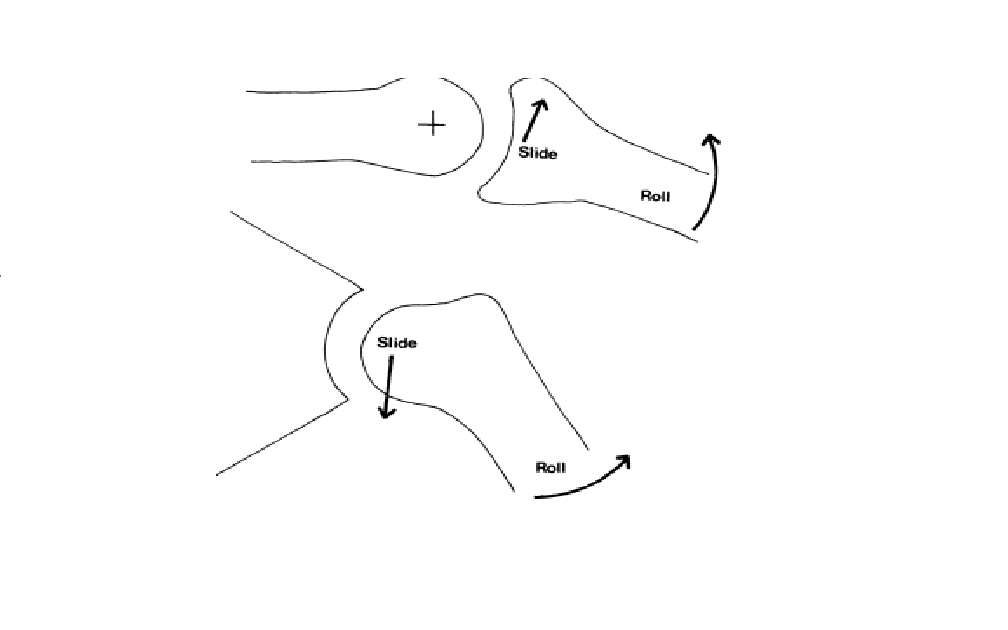 What is fascinating about this evolutional burst is that it happened almost simultaneously in different parts of the world. Freddy Kaltenborn, a physiotherapist from Norway, modified his assessment reasoning based on the application of distractive, compressive and translatory forces on the joints and on how do these joints behave under those forces. Also, he was the one who suggested that certain limitations on the joint movement were directly related with the shape of the joint surfaces (Convex-Concave rule) (Kaltenborn et al., 1999).
What is fascinating about this evolutional burst is that it happened almost simultaneously in different parts of the world. Freddy Kaltenborn, a physiotherapist from Norway, modified his assessment reasoning based on the application of distractive, compressive and translatory forces on the joints and on how do these joints behave under those forces. Also, he was the one who suggested that certain limitations on the joint movement were directly related with the shape of the joint surfaces (Convex-Concave rule) (Kaltenborn et al., 1999).
On the other hand, Geoffrey Maitland approached the application of distractive and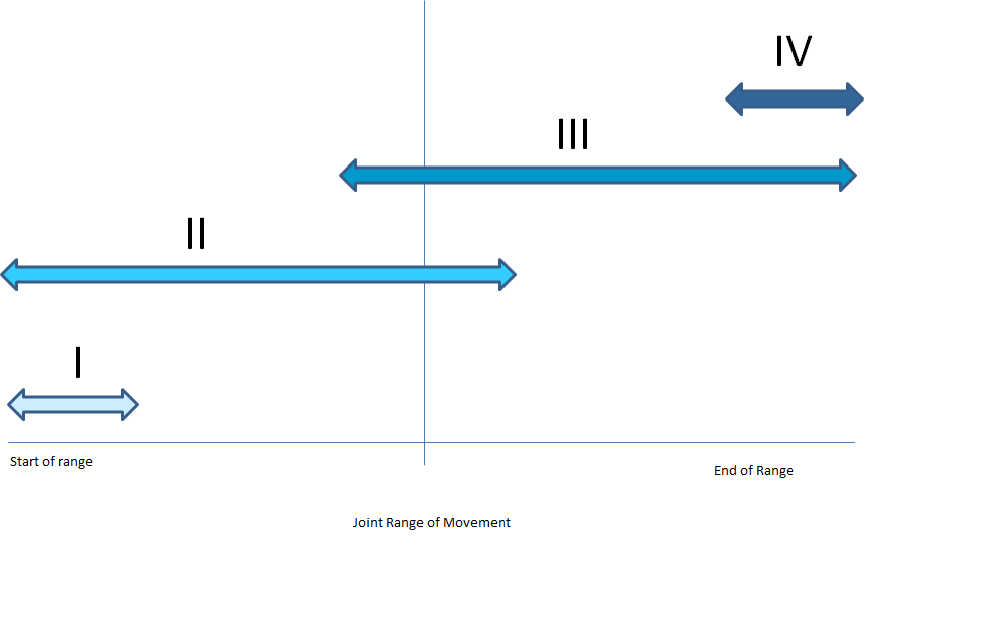 compressive forces to the joints differently. He emphasized on the alleviation of pain rather than only gaining the possibly disturbed range of motion. His clinical reasoning was based on pain response to the passive movement through an appropriately modified assessment procedure. This approach led to the formation of the Grades of Mobilization and the better definition of the terms “Accessory and Physiological Movement” (Maitland et al., 2005). Similarly, Brian Mulligan showed how the application of mobilization during active movements (Mobilization with Movement) can lead to favourable clinical outcomes and how it can also lead to the alleviation of pain (Mulligan, 2010).
compressive forces to the joints differently. He emphasized on the alleviation of pain rather than only gaining the possibly disturbed range of motion. His clinical reasoning was based on pain response to the passive movement through an appropriately modified assessment procedure. This approach led to the formation of the Grades of Mobilization and the better definition of the terms “Accessory and Physiological Movement” (Maitland et al., 2005). Similarly, Brian Mulligan showed how the application of mobilization during active movements (Mobilization with Movement) can lead to favourable clinical outcomes and how it can also lead to the alleviation of pain (Mulligan, 2010).
 These philosophies came to define the practice of manipulation for decades. Of course it doesn’t mean that any of these philosophies and approaches are perfect and to my knowledge none of those extraordinary individuals claimed as such. Ultimately, these methods lay the foundations towards a better, scientifically valid approach of the patient’s problem and consequently increase the effectiveness of the chosen treatment.
These philosophies came to define the practice of manipulation for decades. Of course it doesn’t mean that any of these philosophies and approaches are perfect and to my knowledge none of those extraordinary individuals claimed as such. Ultimately, these methods lay the foundations towards a better, scientifically valid approach of the patient’s problem and consequently increase the effectiveness of the chosen treatment.
Furthermore, those methods, even though they exhibit a form of solidity, they are open to adaptation and to individual perception of any physiotherapist. They are not panaceas. None of the approaches can treat on each own. They are assessment tools to guide the formation of a more effective intervention strategy.
The middle of 20th century was the threshold towards a time of evolution, understanding and practice of manipulation. It is perhaps the first evidence I provide through this blog that by knowing the roots of manipulation, understanding the philosophy and embracing the teachings of the predecessors, a talented individual can reach higher levels of perception, evolve the practice and ultimately achieve transcendence.
References:
Bialosky EJ, Simon BC, Bishop DM, George ZS. Basis for spinal manipulative therapy: A physical therapist perspective. J Electromyogr Kinesiol. 2012; 22(5): 643–647.
Chartered Society of Physiotherapy. History of the Chartered Society of Physiotherapy 2014. In: http://www.csp.org.uk
Huijbregts PA. Orthopaedic Manual Physical Therapy- History, Development, and Future Opportunities. J Phys Ther. 2010; 1:11–24.
Maitland G, Hengeveld H, Banks K, English K. Maitland’s Vertebral Manipulation. Butterworth-Heinemann 2005.
Mulligan B. Manual Therapy: Nags, Snags, MWMs, etc. Orthopedic Physical Therapy Products 2010.
Paris SV. A history of manipulative therapy through the ages and up to the current controversy in the United States. J Manual Manipulative Ther 2000; 8(2):66–77.
Paris SV. In the best interests of the patient. Phys Ther 2006; 86(11):1541–53.
Pettman E. A History of Manipulative Therapy. The Journal of Manual and Manipulative Therapy 2007; 15(3): 165–174.
Wiese G, Callender A. History of spinal manipulation. In: Evans W.D. Why do spinal manipulation techniques take the form they do? Towards a general model of spinal manipulation. Manual Therapy 2010; 15: 212-219
Pictures:
Fig 1: Physiotherapy. In: www.wordofmouth.co.ke
Fig 2: Chartered Society of Physiotherapy. In: www.csp.org.uk
Fig 3: Convex-Concave Rule. In: www.physio-pedia.com
Fig 4: Grades of Mobilization. In: www.physio-pedia.com
Fig 5: Mobilization with Movement. In: www.marshpt.com

Always a pleasure reading your articles Vasilis!! The history of Physiotherapy from a very interesting point of view…